Maternity
Induction of Labour
Patient Information Leaflet
Having your labour induced at Russells Hall Hospital.
Please report concerns about you or your baby’s well-being to maternity triage 01384 456111 extension 3053. Do not wait for your induction time. If you need a translator please call 01384 437934.
CONSENTING TO INDUCTION
It has been explained to me by my doctor, my midwife, or both:
- how the induction process works
- why my doctor believes that induction is the right course of action for me and my baby, and the benefits to me and my baby
- that induction may lead to a prolonged stay in hospital before baby is born so I can prepare things at home accordingly
- that being induced may increase the chance of needing forceps or vacuum-assisted vaginal birth or the chance of needing a caesarean section birth
- that sometimes induction does not work and an alternative plan would need to be agreed with a senior obstetrician
- I know I can ask to speak to a midwife or doctor about my induction at any stage
If you are booked for induction your doctor will complete a personalised induction of labour passport with you outlining your own plan of care.
WHY SHOULD I READ THIS LEAFLET?
You may have already been booked for induction, or you may be looking to find out more about induction of labour as you near the end of your pregnancy. At Russells Hall, and nationally, induction of labour rates are around 35% of all pregnant women at the time this leaflet was written.
If you have been booked for an induction your personalised induction passport will highlight the main reason for your induction and the methods of inducing labour which are appropriate to your specific circumstances.
This leaflet is not intended to replace individualised, one on one conversations about your specific care plan with your doctor or midwife, but gives some general information about the induction process allowing you to plan and understand what to expect when you accept an
induction. Your care plan may deviate from the information in this leaflet if you have specific clinical needs. Not everyone is suitable for induction, your doctor will discuss this with you.
If you have any concerns, it is important that you contact triage if you are not in the hospital on 01384 456111 extension 3053 OR 01384 437934 if you need a translator or use the call bell to call a midwife if you are an in patient if:
• Your waters break
• You have any bleeding
• You are concerned about your baby’s movements
• You have regular, painful contractions
• You cannot pass urine
• You feel unwell or have any sudden onset of pain
INDUCTION TERMINOLOGY (WORDS)
You may hear your care team use some medical terms you don’t hear every day, we have outlined the main ones for you to know below. If you are ever unsure of any terms used please ask your midwife or doctor.

Words referring to body parts:
Uterus/womb – The pear shaped organ where your baby grows during pregnancy.
Amniotic sac – The bag of waters surrounding your baby
Cervix – Neck of the womb. Closed during pregnancy. Opens to 10cm in labour.
Vagina – Muscular tube leading from the cervix to the external genitals.
Medical Words
Dilation / Dilating – Opening. Usually in relation to a cervix as it opens from being closed to 10cm to allow baby to pass through to be born.
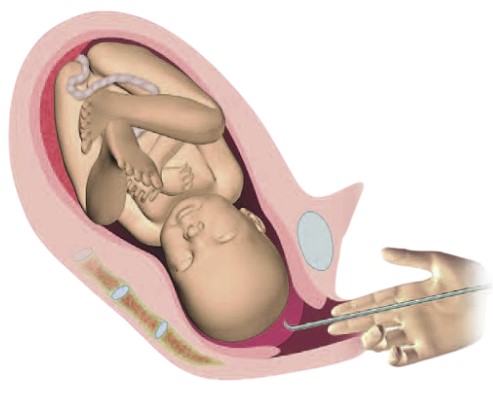
Vaginal examination – Internal assessment of the cervix, using two of the midwife’s fingers, to determine the Bishops’ Score.
Bishop’s Score – A number representing an assessment of the position, firmness and dilation of the cervix to determine the progress of the induction process.
Artificial Rupture of Membranes (ARM) – Also known as amniotomy or breaking waters. All words meaning to break the sac of waters around baby to encourage strong labour contractions to begin.
Speculum – A plastic device inserted into the vagina to allow a doctor or midwife to see your cervix.
Cardiotocograph – Machine that monitors your baby’s heart beat. It will also record any contractions you may be having.
Obstetrician – Doctors specialising in pregnancy. Each day a consultant leads a team of registrars (experienced and senior doctors) who are supported by junior doctors called SHO’s.
Midwife – A specialist nurse trained to facilitate vaginal deliveries, support you during caesarean delivery and to care for your baby after birth.
Anaesthetist – Doctors who when working with pregnant patients specialise in pain relief during labour, providing epidurals for those who want them and ensuring pain relief during caesarean sections.
IS AN INDUCTION RIGHT FOR ME?
Induction is a medical intervention intended to start labour before the body begins itself. Labour usually starts on its own between 37-42 weeks. Induction will be recommended to you when your doctor believes there is a benefit to either your health, the wellbeing of your baby, or both. There are many reasons you may be offered an induction and you should ensure you understand your own personalised reasons for being offered an induction by your doctor or midwife when you accept this. Should you need additional support ask your doctor or midwife for a referral to our consultant midwife. Sometimes you may feel a particular course of action is presented as a given, but remember that you always have choices when it comes to your birth. The BRAIN acronym may help you to think about the benefits, risks and alternatives to any choices or decisions you need to make during your pregnancy and labour.
Questions you could ask….
Benefits:
Why am I being recommended for an induction?
What are the benefits to me of having an induction?
What are the benefits to my baby of an induction?
How does this affect my birth plan/preferences?
Risk:
What are the risks for me of being induced?
What are the risks for my baby of me being induced?
What are my personalised chances of these risks?
What else goes along with me accepting this plan? Other procedures/interventions, fetal monitoring plan etc.
What else changes if I accept?
Alternatives:
Can I decline any specific parts of this plan?
What are my other options and risks/benefits of those?
What else goes along with me accepting this plan? Other procedures/interventions, fetal monitoring plan etc.
Is there a middle ground?
How could I get more options if I’m not comfortable?
Intuition
What does my gut tell me?
What feels right to me?
Can I have some time now to consider my options? How much time/when would we need to make a decision by?
Nothing:
What happens if we do nothing?
What other ways could I and my baby be kept safe?
For how long could we do nothing?
What is the risk of doing nothing?
THE INDUCTION PROCESS
STAGE 1 : DILATING (OPENING) YOUR CERVIX
Your cervix must dilate to 10cm to allow baby to be born. We encourage your cervix to open to around 2cm (size of a penny) for the later stages of the induction process. We can do this by several methods which your doctor will outline in your induction passport when your induction is booked. The most common methods are below and are carried out as inpatient inductions, where you and baby will be regularly monitored and checked. Possible side effects are abdominal discomfort, nausea and vomiting, diarrhoea, abnormally strong contractions of the womb which may cause problems with the baby’s heart rate, vaginal swelling and discomfort or irritation. We will try and make the repeated vaginal examinations as comfortable as possible, but we will ask to assess your cervix at every step of your induction to best manage your plan of care.
One pessary will be placed near your cervix by your midwife. She will use her fingers to do this. The prostaglandin hormones released will encourage your cervix to open. Only one is given and it remains in place for 24 hours.

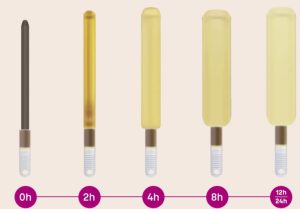
A dose of gel will be placed near your cervix by your midwife using a gel syringe to do this. The prostaglandin hormones released will encourage your cervix to open. We may give a second dose 6 hours later if the first dose has not opened the cervix.

Up to 5 rods inserted through your cervix, the midwife will usually insert these using a speculum. Dilapan rods swell up over this time and open your cervix through both pressure and the natural hormones your body makes in response to this pressure. These remain in place for 24 hours. You may be able to have these rods and to go home for 24 hours to allow them to work, rather than staying in the hospital over the period. Ask your doctor if you are eligible for this outpatient start to the induction process. Studies have shown less pain relief may be needed with this method compared to the hormonal methods.
Before and after all these methods we monitor your baby’s heart rate for at least 40 minutes to assess their wellbeing. We then recommend that you remain upright and mobile as much as possible to allow gravity to help. Once your cervix is around 2cm and has started to move forward and soften and is favourable for the next stage, your midwife will let the midwife in charge know that you are ready to have your waters broken (ARM).
STAGE 2 : BRINGING ON STRONG LABOUR CONTRACTIONS
Once your cervix is favourable enough for us to break your waters you will be taken to a delivery room for one on one care and your second birth partner can come to join you.
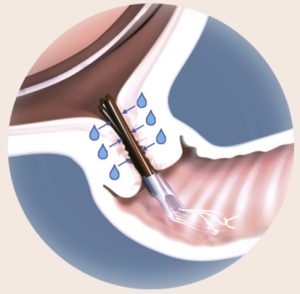
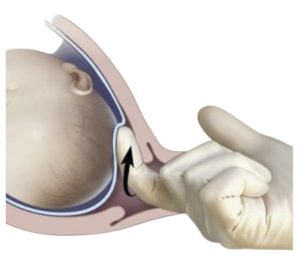
This is also called ARM (artificial rupture of membranes) or amniotomy. We do this using a special plastic tool called an amnihook which has a tiny hook at one end which we use to gently scratch the sac around baby until it opens and allows the amniotic fluid (waters) to come out. If your waters have already broken you would skip this step.
We do this before starting a hormone drip because your waters form a cushion in front of your baby’s head which could slow process. There is a small risk of the umbilical cord prolapsing when the waters are broken but your midwife will only do so once they have checked baby is low, the head is well applied and covering your cervix and they cannot feel a cord in front of baby’s head so that they feel it is safe to continue. If not they will consult a doctor.
BREAKING THE SAC OF WATERS AROUND BABY
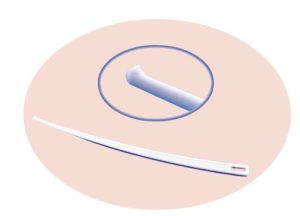 This is also called ARM (artificial rupture of membranes) or amniotomy. We do this using a special plastic tool called an amnihook which has a tiny hook at one end which we use to gently scratch the sac around baby until it opens and allows the amniotic fluid (waters) to come out. If your waters have already broken you would skip this step.
This is also called ARM (artificial rupture of membranes) or amniotomy. We do this using a special plastic tool called an amnihook which has a tiny hook at one end which we use to gently scratch the sac around baby until it opens and allows the amniotic fluid (waters) to come out. If your waters have already broken you would skip this step.
We do this before starting a hormone drip because your waters form a cushion in front of your baby’s head which could slow process. There is a small risk of the umbilical cord prolapsing when the waters are broken but your midwife will only do so once they have checked baby is low, the head is well applied and covering your cervix and they cannot feel a cord in front of baby’s head so that they feel it is safe to continue. If not they will consult a doctor.
SYNTOCINON HORMONE DRIP
Long, strong contractions (around 4 in 10 minutes lasting 90 seconds) are needed to bring your baby through the birth canal and be born. We help you achieve this by giving you a drug called oxytocin through a cannula in your hand to encourage your uterus (womb) to contract regularly and strongly. Long, strong contractions (around 4 in 10 minutes lasting 90 seconds) are needed to bring your baby through the birth canal and be born. We help you achieve this by giving you a drug called oxytocin through a cannula in your hand to encourage your uterus (womb) to contract regularly and strongly.
From this point on we currently recommend that you do not eat and only drink clear fluids such as water or isotonic drinks. We also perform a continuous CTG (monitoring of baby’s heart rate) so that we can see how your baby and your uterus are coping with these strong contractions. Staff are well trained to deal with any complications that arise. When we use hormones to increase/start your contractions, some women report these as being more painful so do consider all the pain relief options open to you to support you as you labour.
INDUCTION TIMESCALES
Inducing labour takes time. Below is an indication of how long your induction process may take. Whilst every labour is different and some may progress more quickly or skip stages it is important to understand how long an induction of labour could potentially take to allow you to prepare mentally and physically and to allow you to plan for child and pet care at home in the meantime. Your primary birth partner can be with you throughout the whole induction, labour and postnatal period.
Stage 1 : Dilating cervix to approx 2cm
1) Hormone pessary or dilapan rods for 24 hours
2) 1st Hormone gel 6 hours
3) 2nd Hormone gel 6 hours
= Up to 36 hours for cervix to be open enough to break waters
+ potential wait of another 24 hours+ for a midwife to be available for waters to be broken to give 1-to-1 labour care*.
*We aim to keep you waiting as short a time as possible for your waters to be broken. You may notice empty rooms but you are waiting for a midwife who is available to care only for you once we break your waters for your safety. Please note :
– Your place in this queue may change depending on the clinical needs of everyone in that queue, including yourself.
– The wait can be unpredictable, for example if there is an unusually high number of spontaneously (naturally) labouring women arriving in triage.
– We recognise this can be frustrating and our lead midwives will keep you up to date with any changes/progress.
Stage 2 : Strong labour contractions
1) Breaking waters
2) Syntocinin hormone drip
Baby is usually born within 12-18 hours
Postnatal (after birth) : 24 hours +
Everyone’s postnatal stay is different depending on their delivery method and any additional checks needed for them or their baby.Some mums and babies will go home within 6 hours and some may be in hospital for a week. Anyone having an induction should plan to be with us for at least 24 hours postnatally. Please ask your doctor or midwife to keep you updated with regards to your own personal timescales, which may alter as your pregnancy and labour progress.
WHAT IF MY INDUCTION DOESN’T WORK?
Sometimes induction does not work if the cervix does not respond to the methods on page 7 and 8. A cervix may not be ready to ripen for labour for a number of reasons, even with encouragement, but this is never your fault. In this case a doctor will discuss next steps with you. They may offer to “rest” you from hormones for some time and then offer a third hormone gel or dilapan rods. This will be tailored to your individual needs and wishes.
Sometimes at this stage you may decide you have tried to be induced but opt for a caesarean section birth instead. Should you decide to opt for caesarean section you will discuss the procedure and timings with an obstetrician (pregnancy doctor) and an anaethetist (who will make sure your pain is controlled during the procedure, usually using spinal analgesia) before making a final decision to proceed.
Occasionally your body may respond too well to the hormones used for induction and you may have more contractions than your baby may safely tolerate. We monitor you closely to pick this up should it happen. We can help you to slow these contractions down and keep a close eye on your baby’s wellbeing on the CTG monitor until things have settled. When this happens a doctor will come and talk to you about slowing the contractions down and about next steps in your induction.
Making informed decisions that are right for you:
Your midwife will be there to support you in your decision making.
It is important to remember that you can change your mind about induction at any time during the process, please just let your midwife know and they will facilitate discussions to allow you to confirm you want to halt the process and to discuss next steps with a obstetrician (pregnancy doctor) about how and when your baby will be born.
THE DAY OF YOUR INDUCTION
If you have any concerns about you or your baby’s well-being please do not wait for your induction time for assessment, please call maternity triage directly on 01384 456111 extension 3053 (or 01384 437934 if you need a translator and find your language code using the QR code on the front page). If you use blood thinners please follow the instructions from your doctor about when to take your last dose before induction as this will cause a delay in the process beginning.
Call 01384 456111 ext 3430 at 10am on the day you have been booked for induction. You will be given a time to arrive to commence your induction* normally between 11am and 8pm. Very rarely your induction may need to be delayed until the next day but we will take steps to ensure you and your baby’s wellbeing if so.
Arrive and check in at reception. You will be directed to your induction bed. This will normally be a 2 bedded room with a shared bathroom.
An induction midwife will carry out a number of admission checks and tests as soon as possible after your arrival. They will also be looking after the ongoing inductions that day so please bear with them if they are not with you right away.
The induction midwife will, with your consent :
- take a blood sample from you
- ask about your and your baby’s wellbeing
- take your temperature, heart rate and blood pressure
- use a CTG machine to trace your baby’s heart
- assess any contraction type pain you may already be having
- ask some questions to admit you on the computer
- assess your cervix and discuss which of the induction types will be most suitable for you and, with your consent, begin the process.
Admission times are allocated based on clinical need and to allow enough time between people to avoid any undue waiting. We are therefore unable to take requests for specific arrival times.
THE DAY OF YOUR INDUCTION – OUTPATIENT
This section is for women who have been booked to have an outpatient induction using dilapan rods only. If you have been booked as an inpatient induction by any method, including dilapan rods please see the previous section. For any issues please call delivery suite directly.
Call 01384 456111 ext 3430 at 10am on the day you have been booked for induction. You will be given a time to arrive to commence your induction* normally between 11am and 8pm. Very rarely your induction may need to be delayed until the next day but we will take steps to ensure you and your baby’s wellbeing if so.
Arrive and check in at reception. You will be directed to your induction bed. This will normally be a 2 bedded room with a shared bathroom.
An induction midwife will carry out a number of admission checks and tests as soon as possible after your arrival. They will also be looking after the ongoing inductions that day so please bear with them if they are not with you right away.
The induction midwife will, with your consent :
- take a blood sample from you
- ask about your and your baby’s wellbeing
- take your temperature, heart rate and blood pressure
- use a CTG machine to trace your baby’s heart
- assess any contraction type pain you may already be having
- ask some questions to admit you on the computer
- assess your cervix and whether you remain suitable for outpatient induction.
With Rods – If you are still suitable for rods and to go home to let them work for 24 hours, the rods will be inserted and a number of safety checks performed before you leave.
For ARM – If you are already dilated enough to have your waters broken then you can usually wait at home and we will call you back when you are at the top of the list, if you are happy to. If you go home at any stage you are not de-prioritised in the queue at all.
Whilst at home please call triage with any concerns at all 01384 456111 extension 3053.
With rods – When you return 24 hours later we will reassess your cervix and whether your waters can be broken or if you need any hormones to encourage further dilation of your cervix.
For ARM – When you are called to return we will break your waters as soon as we can. Please keep your phone on loud as we may call any time of the day/night.
PREPARING FOR THE DAY OF INDUCTION
MEMBRANE SWEEPS
When safe to do so, you may be offered a membrane sweep by your community midwife or at an outpatient appointment before you attend for a planned induction. This may increase the chances of labour starting naturally within the following 48 hours and reduce the need for other methods of induction of labour. Membrane sweeping involves your midwife or, doctor placing a gloved finger just inside your cervix and making a circular, sweeping movement to separate the membranes from the cervix (neck of the womb). If your cervix is closed it will not be possible to perform a membrane sweep.
Membrane sweeping may cause some discomfort or very light bleeding. If you have any questions or concerns after having a membrane sweep, please call Maternity Triage.


BEING READY FOR YOUR INDUCTION AND LABOUR
Good posture – Being upright and sitting forward/leaning forward rather than leaning back can help encourage baby into the best position, this is called “optimal fetal positioning”. For example, try lying/resting on left side, sitting on a chair backwards, or sitting on an exercise ball. Please see more information at nhsforthvalley.com/health-services/az-of-services/maternity/maternityleaflets/advice-for-optimal-fetal-positioning/
Relaxation – The hormones that bring about labour work best when not fighting stress hormones in our body. Whilst some level of nervousness cannot be avoided when coming into the hospital for an induction, arriving calm and relaxed will help your body. Try to do something nice with your partner the night before you arrive to calm. Make sure things are planned at home for childcare / pet sitting and bring things to keep your mind occupied.
Perineal stretching increases the stretchiness and the blood flow of the perineum with the aim of this feeling less painful during birth and tears/episiotomy (a cut to the perineum) less likely. Avoid if you have any urine or vaginal infections or herpes. This video explains how to do this safely: www.kingstonmaternity.org.uk/birth/preparing-labour-and-birth/perineal-health-tears-andepistomies-during-childbirth
What to bring:
- Your hospital bag including comfy clothes and pyjamas
- For baby : vests, grows and cardigans, hats, nappies, muslin cloths, cotton wool/newborn baby wipes, baby blanket if desired though you can leave this in the car if possible until you transfer to a delivery room for space
- Pre-made formula if this is how you plan to feed your baby, we do not have facilities to make up powdered formula.
- The small 6 packs that come with teats are ideal as they are pre-sterilised
- Your primary birth partner! Please bring them food and a small blanket/pillow, they will be in a chair overnight.
- Magazines, colouring books, phone chargers
- Breastfeeding bra if desired
- Maternity pads
- Water bottle/isotonic drinks
- Pain relief items you plan to use : TENS machine, birth comb etc
- As you will be in a shared room think about earphones / ear plugs and a eye mask.
- Any regular medications you take at home, particularly diabetes medication or for any pre-existing conditions, so that we have a supply until we can ensure our own availability of these for you at admission.
- Snacks and drinks (3 meals a day will be provided but only to the pregnant women, partners will not be fed).
- Toiletries (toothpaste, soap, lip balm, shampoo & conditioner, hair ties etc)
What NOT to bring:
- Any analgesia/pain relief (such as paracetamol, codeine etc as we will provide these in the hospital when you need them. We need to know when and what medications you’ve taken when you are with us, to ensure any other medications we need to give you when you are with us are not incompatible or would result in an overdose of a particular drug type).
- Any expensive or sentimental items, such as jewellery and watches, you will be asked to sign a lost property form when you arrive as any such items are brought at your own risk.
- Car seat can stay in the car for now.
- Towels (unless you would prefer to use your own).
- Your second birth partner, they can come along and join you when you go to a delivery room. However they can visit during normal visiting hours, please see security for the most up to date information on visiting hours and number of people visiting at any one time.
If there is anything else you think you may need please ask a midwife who will be happy to advise on your specific circumstances.
PAIN RELIEF FOR LABOUR (ANALGESIA)
Some women report that they need additional pain relief compared to a natural labour as artificial hormones are used to start and maintain strong labour contractions.
At Russells Hall we routinely offer:
- Entonox (Gas and Air) – This is inhaled (breathed in) during contractions. Some women find this helps with the peak of their contraction pain. Some women report this makes them feel woozy/nauseous and it can make their mouth feel dry.
- Pethidine – This is injected into your leg using a needle. Some women find this helps them rest between contractions and eases contraction pain. Some women find this makes them nauseous (feel sick) so we give together with an anti-sickness medication in the same syringe.
Some women worry about it making the baby drowsy at delivery, we will perform checks to ensure you are not expected to deliver rapidly and we will observe baby closely for any signs they may need some antidote (this is exceedingly rare). - Epidural – This is given through a small plastic tube in your back, initially inserted with a needle Some women find this almost entirely removes the pain of contractions, though they can still feel them. An anaesthetist will need to assess if you are suitable for an epidural if you wish for one.
Some women may be able to have a drug called remifentanil through a cannula in their hand as alternative to the above. We recommend keeping an open mind on your pain relief options as every person and every labour is different. Take time to discuss your thoughts and preferences with your birth partners beforehand as they can help you with your decision making during labour, as they know you best.
Two particularly useful documents that compare and discuss pain relief options in more depth :
www.labourpains.org/downloads/english-resources/faqs—pain-relief-in-labour—english.pdf
www.labourpains.org/downloads/english-resources/pain-relief-comparison-card-september-2014.pdf
Labourpains also has this information in 20 different languages at this link
www.labourpains.org/translated-information/overview
Should you wish to know more about induction, please see these websites for credible, research-based information:
The National Institute for Health and Clinical Excellence (NICE) has information for doctors and patients about inducing labour – www.nice.org.uk/guidance/ng207
The NHS – www.nhs.uk/pregnancy/labour-and-birth/inducing-labour/
World Health Organisation recommendations for Induction of labour – iris.who.int/server/api/core/bitstreams/62b11871-9101-4936-9487-db6d1f38c526/content
Our doctors will have discussed the increased likelihood of needing an assisted vaginal delivery (using forceps or a ventouse) and an emergency (unplanned) caesarean section during your consent discussion. They have access to data about rates of these interventions at our hospital which can be tailored to your own situation, please ask them to clarify if needed.
Should you wish for more information on these please see these two information leaftets from the Royal College of Obstetricians and Gynaecologists about these :
Caesarean birth – www.rcog.org.uk/for-the-public/browse-our-patient-information/considering-a-caesarean-birth
Assisted vaginal birth, a vaginal birth using forceps or a ventouse suction cup – www.rcog.org.uk/for-the-public/browse-our-patient-information/assisted-vaginal-birth-ventouse-orforceps
The RCOG have a number of patient information leaflets you may find interesting to supplement what you have read about induction and also through your pregnancy : www.rcog.org.uk/for-the-public/browse-our-patient-information/
Please speak to your doctor or midwife with any questions regarding the above.
If you have any questions, or if there is anything you do not understand about this leaflet, please contact Russells Hall Hospital on 01384 456111.
If you have any feedback on this patient information leaflet, please email dgft.patient.information@nhs.net.
Originator: Charlotte McFarling. Reviewed: July 2026. Next Review Date: July 2029.